Admission TOPIC
On presentation, his oxygen saturation was 92% on ambient air and his blood pressure was 140/85mmHg.
He was awake, aphasic and right-sided hemiplegic with an NIHSS score of 12. Early ischemic changes in the insula region and the precentral gyrus were identified at the emergency plain CT. The patient was admitted in the Stroke Unit of our department under continuous monitoring of vital signs, ECG and BP.
During hospitalization, atrial fibrillation/flutter was not documented. The carotid ultrasound revealed bilateral carotid plaques causing mild stenosis of 30-40%. The transthoracic echocardiography did not reveal any major cardiac abnormality other than heart failure.
During discussions at the ward rounds, the optimal long-term antithrombotic strategy in this patient was discussed. On a pathophysiological basis, thrombi who develop due to low-blood flow (like in the left ventricle due to low ejection fraction) are richer in clotting factors and therefore, may respond better to anticoagulation treatment. In this pathophysiological context, it was suggested that perhaps oral anticoagulation could be the optimal strategy for this patient. However, a recent meta-analysis showed that in patients with HF, any benefit of oral anticoagulation on ischemic outcomes is offset by a significant increase on major bleeds (Ntaios G., Vemmos K. and Lip GYH; Int J Stroke 2019, in press). Our decision was to recommend aspirin (100mg/daily).
🎙️In the final episode of our Spasticity Unlocked series we shift the focus to what matters most: 𝐭𝐡𝐞 𝐩𝐚𝐭𝐢𝐞𝐧𝐭.
Dr. Stevens is joined by Gerard Sewell, offering a powerful & personal perspective on navigating life with #spasticity.
🔢Episodes: https://shorturl.at/F2QYE
#MondayTip
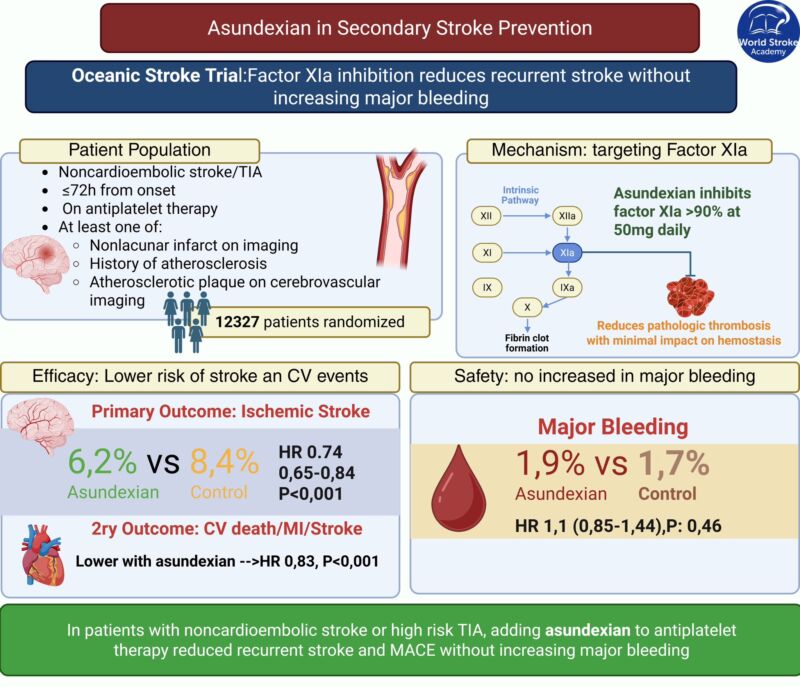
Can we prevent stroke without increasing bleeding?
Factor XIa inhibition #asundexian :
🔹⬇️recurrent stroke (HR 0.74)
🔸with no ⬆️major bleeding in OCEANIC-STROKE.
A potential shift in secondary prevention. 🧠⚖️
🔗 https://www.nejm.org/doi/full/10.1056/NEJMoa2513880
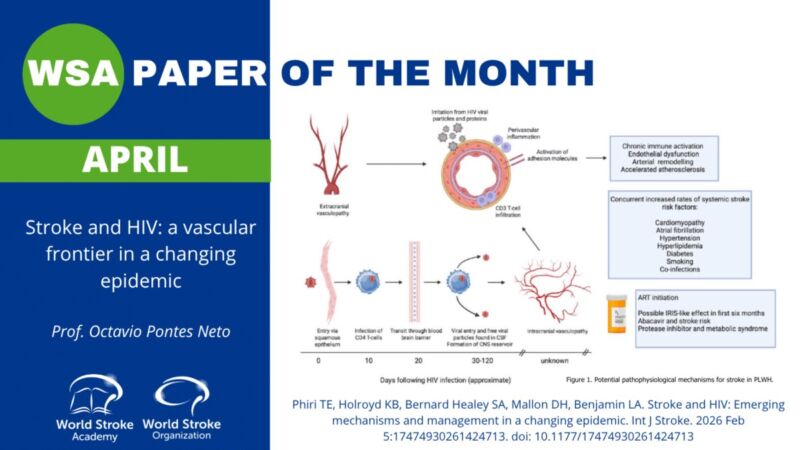
New #PaperOfTheMonth 🔍
🧠Stroke in people living with #HIV is rising & often underrecognized.
🧩A complex mix of
👉vasculopathy
👉inflammation
👉ART effects
👉and traditional risk factors is driving risk at younger ages
Read and listen here ⤵️
https://www.world-stroke-academy.org/news/the-paper-of-the-month-april-5/
🎙️New Episode: Spasticity Unlocked – Treatment Pathways
Practical, patient-centered strategies for smarter spasticity care👥
👉Watch and listen to all episodes here: https://world-stroke-academy.org/news/new-series-spasticity-unlocked-expert-insights-for-clinical-practice-sent/
#StrokeEducation