The Paper of The Month – May
18 May 2026OCEANIC-STROKE: Factor XIa Inhibition Steps into Secondary Stroke Prevention
OCEANIC-STROKE: Factor XIa Inhibition Steps into Secondary Stroke Prevention
Prof. Octavio Marques Pontes-Neto, MD, PhD – Editor-in-Chief, World Stroke Academy
This article is a commentary on the following: Asundexian for Secondary Stroke Prevention. N Engl J Med. 2026 Apr 16;394(15):1467-1479. doi: 10.1056/NEJMoa2513880. PMID: 41985132.
Commentary:
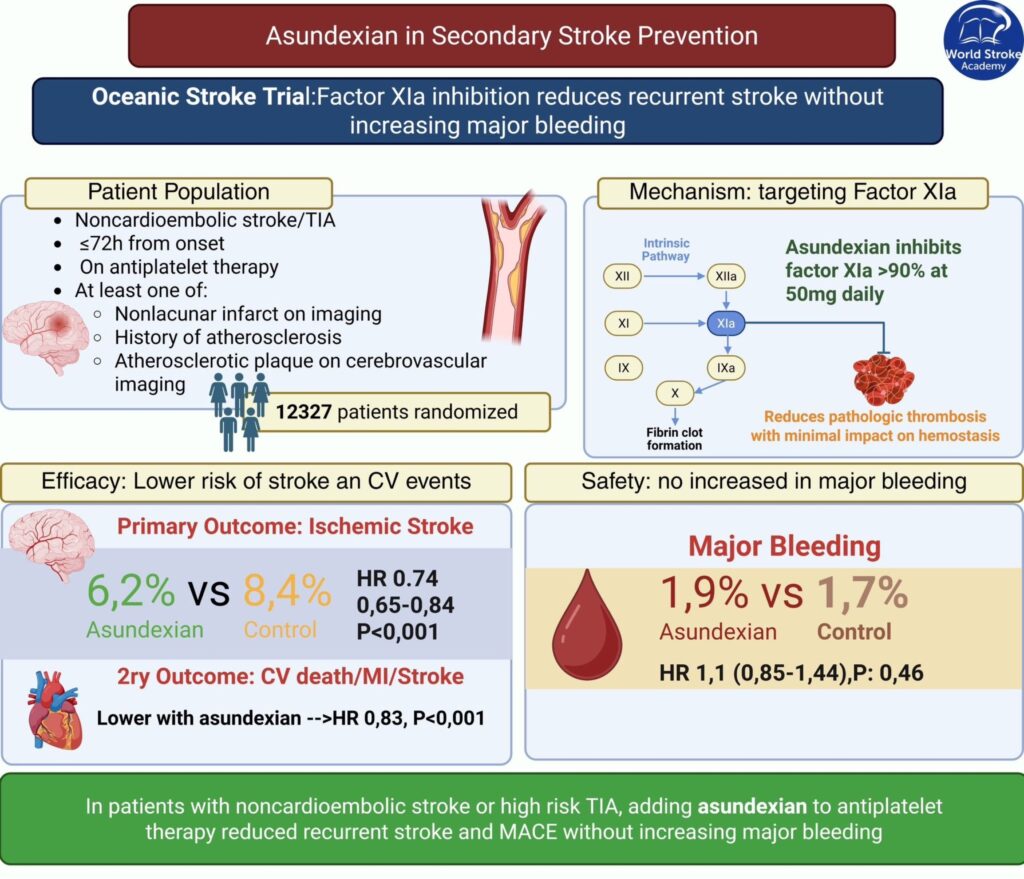
Secondary prevention after noncardioembolic ischemic stroke or high-risk TIA still carries meaningful residual risk. Even with contemporary antiplatelet strategies, including short-term dual antiplatelet therapy followed by monotherapy, recurrent ischemic stroke remains common. Attempts to intensify antithrombotic therapy have repeatedly run into the same barrier: bleeding. The OCEANIC-STROKE trial, published last month in the New England Journal of Medicine, tested a compelling alternative approach by targeting factor XIa, a component of the intrinsic pathway that appears more closely linked to pathologic thrombosis than to essential hemostasis.1 The goal was simple and ambitious: reduce recurrent ischemia without paying the usual bleeding penalty.
This large phase 3, double-blind, randomized trial enrolled 12,327 patients across 702 centers in 37 countries within 72 hours of a noncardioembolic ischemic stroke or a high-risk TIA. Participants were assigned to asundexian 50 mg once daily or placebo, on top of planned antiplatelet therapy. The design intentionally reflected real-world practice. Treating clinicians selected dual or single antiplatelet therapy, and this plan was used as a stratification factor. The population also included the common stroke mechanisms clinicians face daily, including large-artery atherosclerosis and small-vessel occlusion. Most patients had mild strokes at enrollment, with a median NIHSS of 2, and nearly two-thirds were planned for dual antiplatelet therapy, capturing the early period of heightened recurrence risk.
The efficacy result was clear. The primary outcome of ischemic stroke occurred in 6.2% of patients receiving asundexian and 8.4% receiving placebo, with a cause-specific hazard ratio of 0.74 (95% CI, 0.65 to 0.84; P<0.001). Key secondary outcomes moved in the same direction. Any stroke was reduced with a similar relative effect, and the composite of cardiovascular death, myocardial infarction, or stroke was also lower with asundexian. Subgroup analyses were largely consistent, supporting broad applicability across regions and across major noncardioembolic stroke subtypes.
Safety is where OCEANIC-STROKE most strongly differentiates itself from prior combination strategies. ISTH major bleeding was similar between groups, at 1.9% with asundexian and 1.7% with placebo (hazard ratio 1.10; 95% CI, 0.85 to 1.44). Rates of symptomatic intracranial hemorrhage and hemorrhagic stroke were also comparable. This is the dissociation the field has been seeking: fewer ischemic events without an apparent increase in major bleeding when added to antiplatelet therapy.
Some limitations were well acknowledged in the manuscript. The trial included relatively few patients with more severe strokes, only about 5% were enrolled after high-risk TIA, and Black participants were underrepresented. Discontinuation rates were approximately 26% in both groups, which is typical for large prevention trials but still relevant to real-world effectiveness. Yet the core message is difficult to ignore. In a broad noncardioembolic population treated early and predominantly with dual antiplatelet therapy, adding asundexian reduced ischemic stroke and major cardiovascular events without increasing major bleeding.
OCEANIC-STROKE therefore marks na imporant step for secondary stroke prevention. It validates factor XIa as a clinically meaningful target and reopens the conversation about combination antithrombotic therapy, now with a more favorable safety profile than previous attempts. Next steps should focus on translation: identifying patients with the greatest absolute benefit, clarifying the early time-window signal, and defining how factor XIa inhibition fits alongside optimized risk-factor control and etiologic work-up. For now, the trial provides something rare in secondary prevention: a major reduction in ischemic events without a clear major bleeding trade-off.
References:
- Sharma M, Dong Q, Hirano T, Kasner SE, Saver JL, Masjuan J, Demchuk AM, Cordonnier C, Bereczki D, Tsivgoulis G, Veltkamp R, Staikov I, Bae HJ, Campbell BCV, Zini A, Lee IH, Kovar M, Mikulik R, Lemmens R, Ferro JM, Robinson T, Christensen H, Ozturk S, Leker RR, Turcani P, Slowik A, Amaya P, Hoo FK, De Marchis GM, Knoflach M, Sylaja PN, Putaala J, Coutinho JM, van der Worp HB, Miglane E, Matijošaitis V, Lindgren AG, Sampaio Silva G, Sandset EC, Turuspekova ST, Amarenco P, Sheth KN, Smith EE, Eikelboom JW, Joundi RA, Schulze K, Xu L, Heenan L, Colorado P, Keller L, Muehlhofer E, Neumann C, Mundl H, Shoamanesh A; OCEANIC-STROKE Investigators. Asundexian for Secondary Stroke Prevention. N Engl J Med. 2026 Apr 16;394(15):1467-1479. doi: 10.1056/NEJMoa2513880. PMID: 41985132.
Related WSA #MondayTip: