The Paper of The Month – April
17 Apr 2026Stroke and HIV: a vascular frontier in a changing epidemic
Stroke and HIV: a vascular frontier in a changing epidemic
Prof. Octavio Marques Pontes-Neto, MD, PhD – Editor-in-Chief, World Stroke Academy
This article is a commentary on the following: Phiri TE, Holroyd KB, Bernard Healey SA, Mallon DH, Benjamin LA. Stroke and HIV: Emerging mechanisms and management in a changing epidemic. Int J Stroke. 2026 Feb 5:17474930261424713. doi: 10.1177/17474930261424713. Epub ahead of print. PMID: 41644514, https://journals.sagepub.com/doi/10.1177/17474930261424713
Commentary:
Stroke is no longer a rare complication at the margins of HIV care. As Phiri and colleagues argue in a timely review published this month in the International Journal of Stroke, cerebrovascular disease has become a visible and growing contributor to morbidity and mortality among people living with HIV (PLWH), even as antiretroviral therapy (ART) has transformed HIV into a chronic condition. The authors frame the problem with global epidemiologic signals suggesting HIV confers a substantially higher stroke risk, with the overall burden rising as PLWH live longer and age, particularly in sub-Saharan Africa, where both HIV prevalence and health-system constraints intersect.
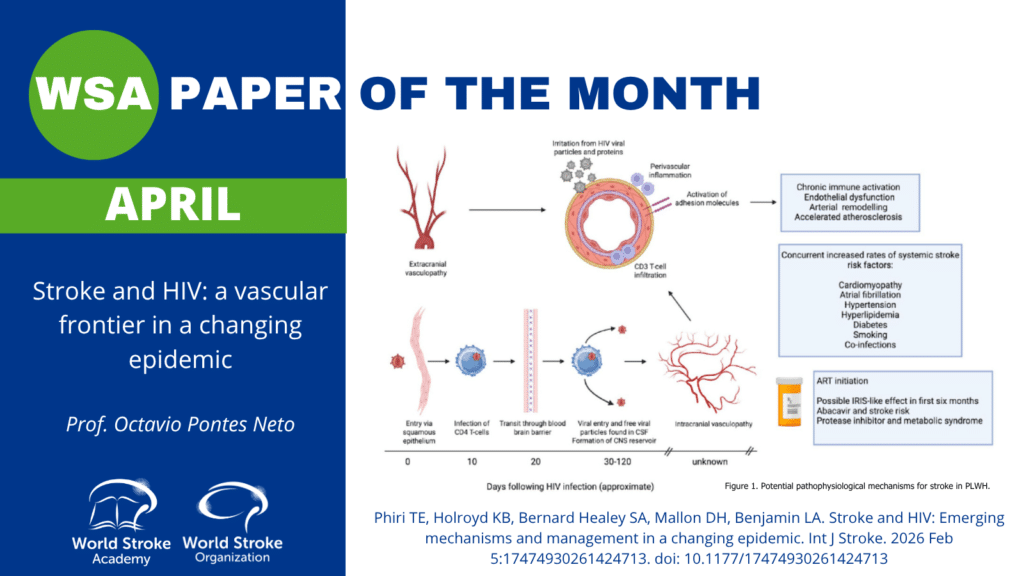
A major strength of the article is its insistence that “HIV-associated stroke” is not a single entity. Instead, stroke mechanisms in PLWH span a continuum, from infection-driven and immune-mediated vascular injury to accelerated vascular aging and atherosclerosis. Stroke mechanisms are also modulated by immune status (CD4 count), viral load, coinfections, and ART exposure. The review highlights vasculopathy as an umbrella that includes inflammatory phenotypes, opportunistic-infection–related vasculitides, and a modern pattern that often resembles accelerated atherosclerosis with distinctive vascular remodeling. It also brings immune reconstitution inflammatory syndrome (IRIS) back into the stroke conversation: in the months after ART initiation or re-initiation, an exaggerated inflammatory response may target the vessel wall, increasing stroke risk in vulnerable patients, especially those with low CD4 nadir and concurrent infection.
Clinically, the message is practical: stroke in PLWH often presents like stroke in anyone else, but it occurs younger, can be multifocal or progressive in vasculopathic phenotypes, and may carry “extra” clues (fever, headache, rash, weight loss, meningitic symptoms) that should trigger a wider differential. The authors provide a useful conceptual framework across HIV disease stages: advanced untreated disease dominated by opportunistic and coinfections; the ART initiation/interruption window where IRIS vasculopathy can emerge; and stable treated HIV where traditional mechanisms (atherosclerosis, small-vessel disease, cardioembolism) reassert themselves, often at an accelerated rate. This staging is particularly valuable in low-resource settings, where careful history-taking may be the most powerful diagnostic tool available.
The review’s approach to investigations is equally actionable and intentionally tiered. Standard acute stroke work-up remains foundational (brain imaging, vascular imaging, cardiac evaluation), but in PLWH the threshold to expand the evaluation should be lower when inflammatory or infectious etiologies are plausible. The authors emphasize cerebrospinal fluid testing when systemic symptoms, inflammatory markers, low CD4 count, or non-atherosclerotic imaging patterns raise suspicion, while also acknowledging that mild CSF pleocytosis can occur in non-infectious stroke, so interpretation must remain cautious. They also recommend incorporating HIV screening into routine stroke evaluation and, for known PLWH with new stroke, documenting CD4 count, viral load, and a minimum screen for key coinfections such as syphilis and tuberculosis.
In hyperacute and secondary prevention management, the paper adopts a balanced tone: reperfusion therapies appear feasible in stable HIV, but evidence is limited and mostly reflects well-controlled disease, while caution is warranted when vasculitis or coinfection-related vasculopathy is suspected due to potential vessel fragility. The authors then highlight a real-world gap that should be uncomfortable for all of us: secondary prevention is under-prescribed in PLWH despite clear indications, and drug–drug interactions (particularly between ART regimens and P2Y12 inhibitors, warfarin, or DOACs) complicate implementation. Rather than discouraging evidence-based therapy, the review pushes clinicians toward deliberate prescribing, choosing compatible agents, monitoring closely, and using established interaction resources, because the alternative is preventable recurrence.
Finally, the review is at its best when it broadens the lens beyond pathophysiology to implementation barriers: stigma, fragmented care, poor access to diagnostics, and clinician awareness gaps, especially in LMICs, shape outcomes as much as biology does. The authors also identify the next research frontier: disentangling whether HIV vasculopathy is distinct or “just faster atherosclerosis,” defining IRIS-stroke epidemiology, mapping small-vessel disease to long-term cognitive decline, and understanding intracranial (CNS-reservoir) mechanisms that peripheral biomarkers cannot capture. The take-home message for the World Stroke Academy community is clear: stroke and HIV is now a mainstream stroke topic. Clinicians should maintain a high index of suspicion, build stage-informed diagnostic pathways, and deliver equitable access to proven prevention, while the research community closes the mechanistic and outcomes gaps that still limit truly evidence-based care.
References:
- Phiri TE, Holroyd KB, Bernard Healey SA, Mallon DH, Benjamin LA. Stroke and HIV: Emerging mechanisms and management in a changing epidemic. Int J Stroke. 2026 Feb 5:17474930261424713. doi: 10.1177/17474930261424713. Epub ahead of print. PMID: 41644514, https://journals.sagepub.com/doi/10.1177/17474930261424713