The Paper of The Month – June
24 Jun 2026TRIDENT: A Simple Triple Pill to Prevent Recurrent Stroke After Intracerebral Hemorrhage
TRIDENT: A Simple Triple Pill to Prevent Recurrent Stroke After Intracerebral Hemorrhage
Prof. Octavio Marques Pontes-Neto, MD, PhD – Editor-in-Chief, World Stroke Academy
This article is a commentary on the following: Three Low-Dose Antihypertensive Agents in a Single Pill after Intracerebral Hemorrhage. N Engl J Med. 2026 Apr 23;394(16):1571-1582. doi: 10.1056/NEJMoa2515043. PMID: 42019018.
Commentary:
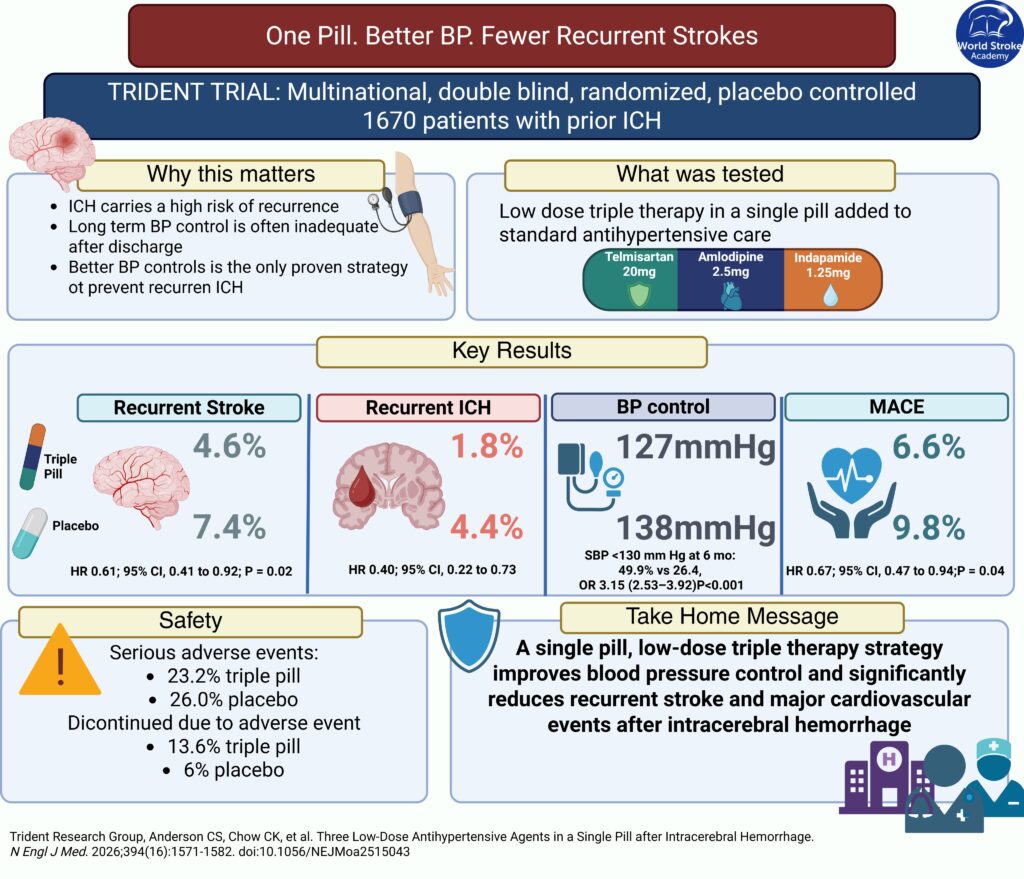
Long-term prevention after intracerebral hemorrhage remains one of the most challenging areas in stroke medicine. Unlike ischemic stroke, for which several antithrombotic and lipid-lowering strategies are available, effective blood-pressure control remains the only proven intervention to reduce the risk of recurrent intracerebral hemorrhage. Yet in routine practice, sustained control is frequently inadequate because of therapeutic inertia, poor adherence, uncertainty about treatment targets, and the complexity of multidrug regimens. The TRIDENT trial addressed this implementation gap by asking whether a single pill combining three low-dose antihypertensive agents could improve blood-pressure control and reduce recurrent stroke after intracerebral hemorrhage.1
TRIDENT was a multinational, double-blind, randomized, placebo-controlled trial conducted at 61 sites in 12 countries.1 After a two-week active run-in period, 1,670 clinically stable patients with previous spontaneous intracerebral hemorrhage and a systolic blood pressure between 130 and 160 mm Hg were randomly assigned to receive either a once-daily triple pill or matching placebo, in addition to usual antihypertensive care. The combination contained low doses of telmisartan, amlodipine, and indapamide, three agents with complementary mechanisms of action. Randomization occurred a median of approximately 54 days after the qualifying hemorrhage, and patients were followed for a median of 2.5 years.
The results were clinically relevant. Recurrent stroke occurred in 4.6% of patients assigned to the triple pill and 7.4% of those receiving placebo, corresponding to a 39% relative reduction in risk and a hazard ratio of 0.61. The estimated number needed to treat to prevent one recurrent stroke was 35. The benefit appeared to be driven predominantly by a reduction in recurrent intracerebral hemorrhage, which occurred in 1.8% of patients in the triple-pill group and 4.4% in the placebo group. Major cardiovascular events were also less frequent with the triple pill, at 6.6% compared with 9.8%. These findings reinforce the strong relationship between blood pressure and recurrent hemorrhagic stroke.
The effectiveness of the intervention was supported by a substantial and sustained difference in blood pressure. Mean systolic blood pressure during follow-up was 127 mm Hg in the triple-pill group and 138 mm Hg in the placebo group, despite the use of background antihypertensive therapy in both groups. At six months, almost half of the patients receiving the triple pill had achieved a systolic blood pressure below 130 mm Hg, compared with approximately one quarter of those receiving placebo. The trial therefore demonstrates not only the benefit of more intensive blood-pressure reduction, but also the practical value of a fixed-dose combination in simplifying treatment and potentially reducing therapeutic inertia.
Safety requires careful interpretation. Serious adverse events were not increased with the triple pill, but discontinuation of the study regimen because of adverse events was more frequent, mainly because of protocol-mandated withdrawal after a rise of 20% or more in serum creatinine. The authors note that this threshold may have been overly conservative, since current evidence generally supports a higher threshold before treatment modification is required. Hypotension also led to more discontinuations, although severe renal outcomes and progression of chronic kidney disease were not increased. These findings emphasize the importance of monitoring renal function and treatment tolerance during treatment initiation and follow-up.
Some limitations were appropriately acknowledged. Most participants were recruited in Sri Lanka, which may affect generalizability, and the active run-in phase selected patients who could tolerate and adhere to the regimen before randomization. Nevertheless, the blood-pressure effect was consistent across countries and demographic subgroups, and the primary result remained robust across sensitivity analyses. TRIDENT provides clinically relevant evidence that a fixed-dose, low-dose combination may improve long-term blood-pressure control and reduce recurrent stroke after intracerebral hemorrhage. Its most important contribution may be the demonstration that treatment simplification can help close the gap between guideline recommendations and sustained blood-pressure control in clinical practice.
Disclosure: The author of this editorial was an investigator and coauthor of the TRIDENT trial.
References:
- Trident Research Group; Anderson CS, Chow CK, de Silva HA, Senanayake B, Wahab K, Al-Shahi Salman R, Klijn CJM, Martins SO, Espinosa N, Kuhles L, Billot L, Arima H, Carcel C, Wang X, Li Q, Shan S, Shanthakumar M, Nguyen HT, Palliyaguruge D, Peiris J, Ranawaka UK, Bandusena S, Rajendiran T, Wijegunasinghe D, Gunasekera H, Wijeweera I, Dissanayake A, Keshavaraj A, Obiako RO, Akinyemi R, Nasi L, Bazan R, Moro CHC, Battaglini M, Zétola V, Law WC, Chia YK, Cordato D, Grimley R, Dahanayaka A, Liyanagamage S, Fernando N, Rasheed NA, Kakabadze N, Beridze M, Aravinthan M, Sahathevan V, Wijesundara D, Ruwanpathirana P, Wan Zaidi WA, Kherkheulidze T, Fischer U, de Souza AC, Lee TH, Chen C, Pontes-Neto O, Robinson T, Wang J, Naismith SL, Barnett M, Delfino C, You S, Liu F, Delcourt C, Moullaali TJ, Wilkinson T, Watson N, Santo K, Han Q, Souza MA, Jolink WMT, Cristofari AB, Zhou Z, Schreuder FH, Lindley RI, Armenis M, Woodward M, Freed R, Song L, Chalmers J, Rodgers A. Three Low-Dose Antihypertensive Agents in a Single Pill after Intracerebral Hemorrhage. N Engl J Med. 2026 Apr 23;394(16):1571-1582. doi: 10.1056/NEJMoa2515043. PMID: 42019018.
Related Webinar:
Hypertension and Intracerebral Hemorrhage: From Acute Blood Pressure Control to Long-Term Prevention
Related WSA #MondayTip: