The Paper of The Month – March
17 Mar 2026Addressing Sex and Gender Differences in Stroke Risk and Management: From Describing Disparities to Delivering Equity
Addressing Sex and Gender Differences in Stroke Risk and Management: From Describing Disparities to Delivering Equity
Prof. Octavio Marques Pontes-Neto, MD, PhD – Editor-in-Chief, World Stroke Academy
This article is a commentary on the following: Addressing sex and gender differences in stroke risk and management: A scientific statement from the World Stroke Organization. Int J Stroke. 2026 Mar;21(3):303-323. doi: 10.1177/17474930251393009. Epub 2025 Oct 23. PMID: 41131690.
Commentary:
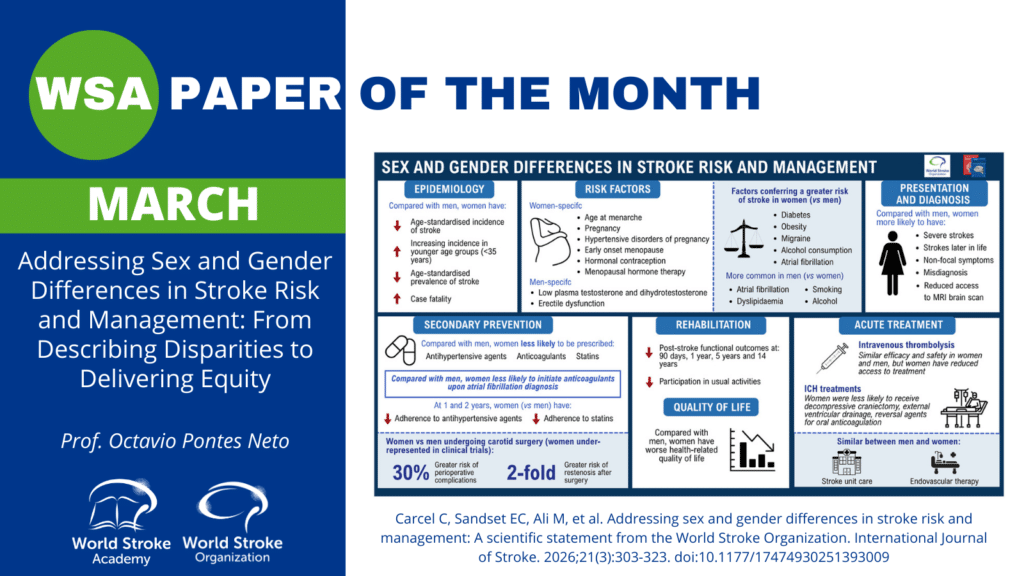
The new World Stroke Organization Scientific Statement by Carcel and colleagues is a timely and pragmatic call to action: sex- and gender-related differences are not a side note in stroke medicine. They are a core determinant of who has a stroke, how quickly stroke is recognized, what treatments are delivered, and what recovery looks like. The statement carefully distinguishes sex (biological, hormonal, genetic influences) from gender (social, behavioral, cultural influences), while acknowledging that most real-world datasets still blend both concepts and remain largely binary, leaving major evidence gaps for transgender, non-binary, and intersex populations.
A major strength of the document is its life-course framing of risk. It synthesizes epidemiologic data showing that overall age-standardized stroke incidence and mortality are higher in males, yet women carry a disproportionate burden at the extremes of age, with higher stroke risk in the youngest adults and again in the oldest groups, where longevity and comorbidity converge. Beyond the shared vascular drivers (hypertension, atrial fibrillation, diabetes, obesity), the statement emphasizes that women experience stroke risk modifiers that are often under-elicited in routine history-taking: hypertensive disorders of pregnancy, gestational diabetes, preterm delivery and other adverse pregnancy outcomes, menopause timing, and exposure to exogenous hormones (contraception and menopausal hormone therapy). These exposures are not merely “obstetric history”. They are actionable vascular risk signals that should trigger earlier prevention, tighter risk-factor control, and longitudinal follow-up.
The statement is also direct about a critical paradox in modern stroke care: when women receive evidence-based acute therapies, benefits are comparable to men, yet women are less likely to receive timely acute treatment. One contributor is diagnostic friction: women are more likely to present with non-focal or less typical symptoms (e.g., altered consciousness, generalized weakness, headache), increasing the risk of misdiagnosis in prehospital and emergency department settings. Another contributor is systems performance: across multiple datasets, women have lower odds of receiving intravenous thrombolysis in routine practice, even though trial and pooled analyses do not suggest meaningful sex-based differences in treatment efficacy when therapy is delivered.
Importantly, the authors move beyond describing the problem and propose a solutions agenda that is highly implementable. They recommend gender-responsive prevention and care pathways that systematically incorporate pregnancy-related and menopausal factors into risk assessment; targeted education for health professionals and the public to improve symptom recognition in women; and stroke quality programs that explicitly track sex-disaggregated process metrics (for example, eligibility, offer, and receipt of reperfusion therapies, and treatment times) to identify where inequities arise and to drive accountability. The statement also highlights adherence as a practical equity lever: women are less likely to be prescribed and to persist with key secondary prevention therapies in several cohorts, and they may experience adverse effects that reduce adherence, which argues for proactive counseling, pharmacist-supported follow-up, and personalized management rather than assuming “one prescription equals one outcome.”
Finally, the research message is unambiguous: equity requires evidence. The statement calls for purposeful inclusion of women across the research continuum and for routine sex- and gender-disaggregated reporting, particularly in areas where practice decisions still rely on underpowered subgroup analyses (procedural risks, dosing, safety, rehabilitation outcomes, and long-term quality of life). It also underscores that sex and gender intersect with race, geography, and socioeconomic status, and that LMIC data are particularly sparse, meaning that global stroke equity will not be achieved by extrapolating from a narrow evidence base.
For clinicians and stroke systems, the take-home is practical: start by asking the right risk questions (including pregnancy and menopause history), design pathways that recognize diagnostic bias and atypical presentations, measure performance by sex, and close the gap between “available” and “delivered” treatment. For the World Stroke Organization community, this statement is a blueprint for translating equity from principle into protocols and for ensuring that excellent stroke care is excellent for everyone.
References:
- Carcel C, Sandset EC, Ali M, Allende Echanez MI, Mosconi MG, de Souza AC, Dalli LL, Venturelli PM, Sakamoto Y, Nasreldein A, Yu AY, Walter S, Lannin NA, Drummond A, Caso V, Alladi S, Bushnell CD, Reeves MJ, Gall S. Addressing sex and gender differences in stroke risk and management: A scientific statement from the World Stroke Organization. Int J Stroke. 2026 Mar;21(3):303-323. doi: 10.1177/17474930251393009. Epub 2025 Oct 23. PMID: 41131690.